Healthcare organizations modernizing their digital infrastructure eventually face a critical architectural decision. Should they build custom integration infrastructure tailored specifically to their workflows, or should they rely on middleware platforms that promise faster connectivity between existing systems?
At first glance, middleware looks like the obvious answer. It promises faster deployment, prebuilt connectors, reduced engineering effort, and simplified integration management. For organizations under pressure to improve interoperability quickly, this approach feels practical and low risk.
But healthcare architecture rarely stays simple for long.
That is exactly why organizations evaluating long-term medical system integration need to think beyond implementation speed and focus on scalability, flexibility, governance, and long-term operational control.
The real question is not whether middleware works.
The real question is whether it will still work once the organization becomes more complex.
Why Middleware Looks Attractive at the Beginning
Middleware platforms are designed to solve a familiar problem. Most organizations operate multiple disconnected systems that need to exchange information without requiring every platform to connect directly to every other platform.
Instead of building custom infrastructure, middleware acts as the communication layer between systems. Data flows through a central orchestration platform that manages connectors, message routing, retries, monitoring, and workflow automation.
That creates clear advantages.
Implementation is usually faster because common systems may already have prebuilt connectors. Internal engineering teams take on less technical responsibility because the vendor manages much of the platform infrastructure. Monitoring tools, dashboards, and operational workflows often come included. Initial project risk feels lower because less custom development is required.
For relatively straightforward interoperability requirements, this can be an excellent solution.
A healthcare provider connecting CRM workflows to appointment scheduling, billing visibility, and standard notification systems may achieve strong results with middleware. A telehealth company trying to integrate with a limited number of supported platforms may move much faster using prebuilt infrastructure instead of custom engineering.
For smaller organizations, speed matters.
For pilot programs, speed matters even more.
That is why middleware often becomes the default starting point.
Where Healthcare Complexity Changes the Equation
The challenge is that healthcare interoperability rarely remains limited to simple connector logic.
Healthcare systems are operationally messy.
A hospital network may operate multiple EHR environments inherited through acquisitions. A specialty provider may depend on vendor software with weak API support. A telehealth platform may require custom synchronization rules for clinical continuity. Identity management may require advanced patient matching across inconsistent records. Governance requirements may demand highly specific access controls, consent workflows, and audit visibility.
At this point, middleware starts showing limitations.
Middleware platforms work best when workflows fit comfortably inside their architectural assumptions.
Healthcare frequently does not.
Clinical operations are not generic automation pipelines. They involve treatment continuity, diagnostics coordination, referral routing, claims workflows, compliance oversight, security governance, and patient identity integrity.
If the organization must constantly bend its workflows to fit middleware limitations, the initial convenience becomes expensive.
This is where the conversation changes from "how fast can we connect systems?" to "how much architectural control do we actually need?"
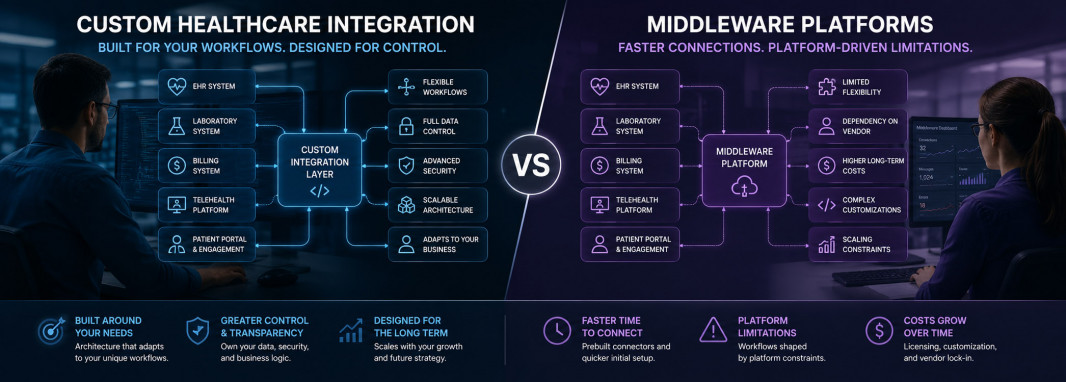
The Biggest Difference Is Control
The core distinction between middleware and custom integration is simple.
Middleware optimizes for speed.
Custom integration optimizes for control.
That difference becomes more important as infrastructure complexity grows.
A middleware platform gives organizations faster access to prebuilt orchestration capabilities, but those capabilities exist inside someone else's architectural model. Authentication logic, connector behavior, transformation flexibility, workflow orchestration depth, security implementation options, and scaling constraints are all influenced by platform design decisions.
Custom integration works differently.
The organization owns the architecture.
That means complete control over data movement, transformation logic, identity reconciliation, security models, governance workflows, monitoring infrastructure, scaling strategy, and interoperability evolution.
That level of control matters much more in healthcare than in many other industries.
Healthcare systems evolve constantly. Vendors change APIs. New software gets introduced. Business units expand. Acquisitions happen. Compliance expectations shift. Clinical workflows adapt.
Rigid infrastructure becomes painful very quickly.
The Hidden Cost of Middleware Dependency
Middleware often looks financially efficient early in the process.
Implementation appears cheaper because engineering effort is reduced.
That calculation is often incomplete.
As complexity increases, middleware costs can expand significantly. Licensing fees grow. Premium connectors require additional spending. Vendor professional services become necessary for advanced customization. Workflow logic becomes harder to manage. Teams become dependent on platform-specific operational knowledge.
Over time, organizations may discover they are not simply paying for middleware.
They are paying for dependency.
Migration becomes harder because business logic increasingly lives inside platform-specific orchestration.
This is a softer form of vendor lock-in.
The organization technically retains flexibility, but practically becomes deeply tied to middleware architecture.
Healthcare organizations planning long-term modernization need to account for this.
Fast implementation today can create strategic constraints tomorrow.
Where Custom Integration Wins
Custom healthcare integration requires more effort upfront.
Architecture design takes longer. Engineering investment is higher. Governance ownership becomes internal responsibility. Testing complexity increases. Monitoring infrastructure must be built deliberately.
That is all true.
But in exchange, organizations gain architectural freedom.
Custom integration allows workflows to reflect operational reality instead of platform assumptions. Security architecture can be designed around internal governance requirements. Identity resolution can follow organization-specific logic. Data transformation can support complex normalization requirements. Legacy infrastructure can be accommodated without waiting for vendor roadmap support.
This becomes particularly valuable in larger healthcare ecosystems.
Multi-location provider networks, enterprise healthcare groups, hybrid clinical environments, specialty care organizations, and digitally ambitious healthcare businesses rarely remain stable enough for generic architectural assumptions to stay useful forever.
Custom integration evolves alongside business strategy.
That flexibility creates long-term leverage.
Hybrid Models Often Make the Most Sense
This is not always a binary decision.
Some mature healthcare organizations combine both approaches effectively.
Middleware handles commodity connectivity where prebuilt workflows provide obvious efficiency. Standard CRM synchronization, messaging automation, scheduling workflows, and lightweight interoperability may fit perfectly inside middleware infrastructure.
Custom integration handles strategic architecture where flexibility matters more.
Complex patient identity management, data aggregation, security-sensitive orchestration, analytics normalization, and organization-specific clinical workflows often benefit from custom infrastructure ownership.
This hybrid approach can be highly effective when architectural boundaries are clearly defined.
The mistake is assuming middleware solves all interoperability problems permanently.
It solves specific categories of integration problems well.
Healthcare modernization is a broader architecture challenge.
The Right Decision Depends on the Future, Not Today
Organizations often evaluate this decision based on immediate implementation convenience.
That is the wrong lens.
The better question is much simpler.
What will this architecture look like in three years?
If the organization expects relatively stable workflows, predictable software environments, and limited integration complexity, middleware may be the right answer.
If the organization expects growth, evolving interoperability demands, acquisitions, governance complexity, deeper analytics needs, AI readiness requirements, or expanding digital healthcare capabilities, custom integration becomes much more compelling.
Healthcare interoperability is not a connector problem.
It is an infrastructure strategy problem.
The strongest organizations choose architecture based not on what feels easiest now, but on what continues supporting the business once complexity inevitably arrives.



