
Healthcare decision makers exploring interoperability inevitably encounter the same acronyms over and over again: HL7 and FHIR. They are often discussed as though they are competing technologies where one simply replaces the other, but that framing creates confusion and poor strategic decisions.
The reality is much more nuanced.
Organizations investing in modern healthcare interoperability often assume the conversation is simply about choosing the newer standard. In practice, the architectural decision is more complex because HL7 and FHIR emerged in different technological eras, solve different integration challenges, and continue to coexist inside real healthcare ecosystems. A modern healthcare interoperability solution rarely ignores either standard entirely.
Why HL7 Still Exists Everywhere
HL7 has been part of healthcare infrastructure for decades. It became the backbone of interoperability in an era when healthcare systems needed a standardized way to exchange structured messages between enterprise applications. Hospitals, laboratories, billing platforms, radiology systems, pharmacy workflows, and countless internal healthcare applications adopted HL7-based communication because it solved a real problem at the time.
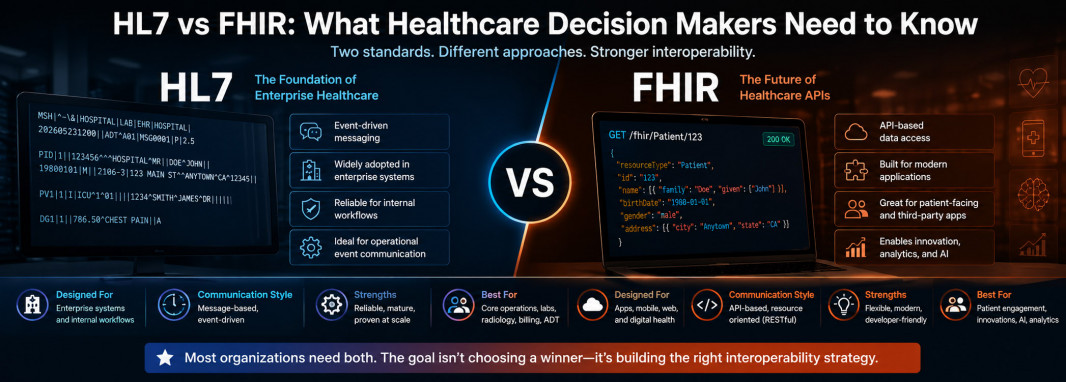
The key thing decision makers need to understand is that HL7 was designed for enterprise messaging, not for modern web-native application ecosystems.
In practical terms, HL7 works by transmitting structured messages between systems when events happen. A patient is admitted. A lab order is created. A diagnostic result becomes available. A discharge occurs. One system generates a message, another system receives it, interprets the data, and updates its own records accordingly.
This model remains extremely common across enterprise healthcare infrastructure.
That is why HL7 still exists almost everywhere.
Large hospitals often depend on legacy infrastructure deeply integrated around HL7 messaging workflows. Laboratory systems still rely on HL7 communication. Billing environments may depend on HL7 event logic. Internal operational workflows across mature provider organizations frequently continue using it because replacing those architectures is expensive, risky, and operationally disruptive.
HL7 survives because healthcare infrastructure does not reset every five years.
Why FHIR Changed the Conversation
FHIR emerged because healthcare interoperability needed a more modern architectural model.
While HL7 evolved in an enterprise systems era, FHIR was designed for API-driven ecosystems where applications need cleaner, more flexible, web-native access to healthcare information.
This difference matters enormously.
Instead of event-driven message passing as the primary model, FHIR exposes healthcare data as structured resources that can be requested, updated, and exchanged through APIs using modern web standards.
That means applications can request patient records, medication history, appointments, allergies, diagnostic results, care plans, and other structured healthcare data in a way that feels much closer to modern software development expectations.
For digital health companies, telemedicine platforms, mobile healthcare apps, analytics products, AI systems, and patient engagement platforms, this changes everything.
FHIR makes interoperability dramatically more developer-friendly.
That does not automatically make it universally superior.
It simply makes it better aligned with modern integration models.
HL7 vs FHIR Is Really a Question of Architecture
Decision makers often ask which standard is better.
That is usually the wrong question.
The better question is what kind of interoperability architecture the organization actually needs.
HL7 is fundamentally message-driven.
FHIR is fundamentally resource-driven and API-oriented.
HL7 excels when enterprise systems need structured event communication between mature operational platforms.
FHIR excels when modern applications need flexible, real-time access to healthcare data.
A hospital laboratory workflow pushing result notifications internally may function perfectly well through HL7 messaging.
A patient-facing digital health application requesting medication history through an API is much better aligned with FHIR.
This is why real healthcare environments rarely operate as pure HL7 or pure FHIR ecosystems.
They operate as hybrids.
Why FHIR Does Not Instantly Replace HL7
This is one of the biggest misconceptions in healthcare technology.
FHIR is newer.
FHIR is cleaner.
FHIR is easier for modern developers.
None of those facts automatically eliminate HL7.
Healthcare organizations carry massive infrastructure debt.
Replacing mature enterprise healthcare systems is expensive. Critical workflows depend on existing integrations. Internal vendor ecosystems often remain deeply tied to HL7 messaging models. Some operational platforms expose limited or incomplete FHIR support while still relying heavily on HL7 internally.
Supporting FHIR on a product brochure does not always mean meaningful production interoperability exists.
Decision makers need to be skeptical here.
A vendor may technically support FHIR while exposing only a narrow subset of useful endpoints. Authentication models may be weak. Data models may be inconsistent. API rate limitations may create operational constraints.
FHIR maturity varies significantly across vendors.
That means architectural evaluation still matters.
What Business Leaders Should Actually Care About
Technical acronyms are easy to get lost in.
Healthcare leadership should focus on business implications instead.
The real questions are operational.
Will the interoperability model support current workflows?
Can it scale as the organization grows?
Will new digital initiatives integrate cleanly?
How difficult is vendor onboarding?
Can analytics platforms access normalized structured data?
Will AI systems get reliable access to usable information?
How expensive is long-term maintenance?
How much vendor dependency does the chosen architecture create?
These questions matter far more than abstract protocol debates.
A legacy hospital network with deeply embedded enterprise workflows may need strong HL7 support for operational continuity.
A digital-first healthcare company building modern patient experiences may prioritize FHIR-native architecture aggressively.
A growing enterprise provider may need both.
The Hybrid Future Is the Most Realistic One
The most realistic architectural model for many healthcare organizations is not choosing HL7 or FHIR.
It is designing infrastructure that accommodates both intelligently.
HL7 may continue handling internal enterprise event workflows.
FHIR may power modern API access layers.
Middleware or interoperability platforms may translate between environments.
Identity resolution layers may normalize fragmented patient data across both standards.
Analytics and AI platforms may consume structured normalized information above the protocol layer entirely.
That hybrid architecture reflects real-world healthcare better than simplistic replacement narratives.
Healthcare modernization rarely happens through clean technical resets.
It happens through layered transformation.
Strategic Takeaway for Decision Makers
Decision makers should stop viewing HL7 versus FHIR as a winner-takes-all technology comparison.
HL7 represents decades of embedded enterprise healthcare infrastructure that still powers critical operational workflows.
FHIR represents the architectural direction of modern healthcare interoperability, particularly for API-driven ecosystems, digital health innovation, analytics, and AI readiness.
The strongest organizations make interoperability decisions based on business architecture rather than acronym hype.
If the objective is preserving mature internal workflows while modernizing gradually, HL7 remains highly relevant.
If the objective is scalable modern interoperability, external ecosystem integration, patient-facing innovation, and future-ready healthcare architecture, FHIR becomes increasingly essential.
For most serious healthcare organizations, the answer is not replacement.
It is controlled coexistence with a clear modernization strategy.



