Healthcare APIs are often marketed as the long-awaited solution to interoperability problems. Vendors showcase FHIR compatibility, developer portals, API documentation, and integration-ready platforms as proof that healthcare connectivity has finally become straightforward. From a business perspective, the promise sounds compelling. If systems expose APIs, then EHRs should connect cleanly with telehealth platforms, billing systems should synchronize automatically, patient engagement tools should exchange information seamlessly, and healthcare organizations should finally escape the inefficiencies caused by fragmented infrastructure.
Reality is significantly more complicated.
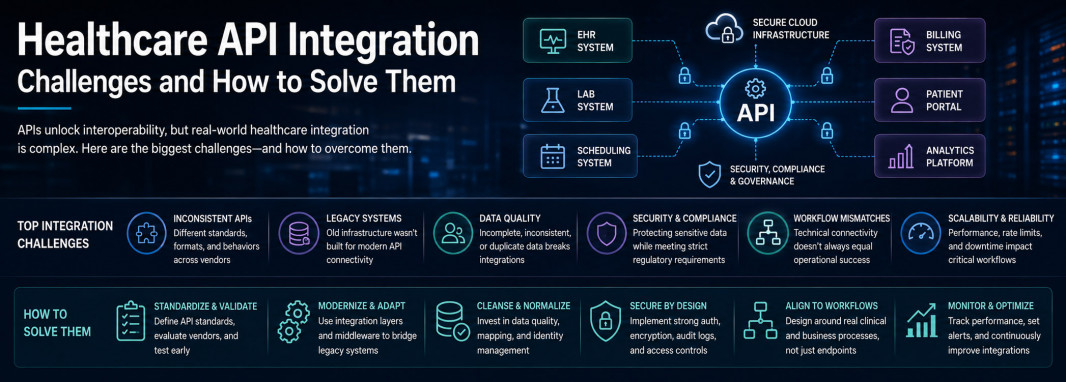
Organizations pursuing a modern healthcare interoperability solution quickly discover that API connectivity solves only one part of the broader challenge. The technical ability to exchange data does not automatically create operational interoperability, reliable workflows, trustworthy patient records, or scalable digital healthcare ecosystems. Successful API integration requires dealing with messy vendor ecosystems, legacy infrastructure, security constraints, inconsistent healthcare data, and architectural complexity that API documentation alone rarely reveals.
API Access Does Not Automatically Mean Integration Readiness
One of the most common mistakes healthcare decision-makers make is assuming that the phrase "API support" means a platform is genuinely ready for interoperability.
In procurement conversations, API availability sounds reassuring because it suggests openness, flexibility, and technical maturity. In practical engineering work, however, API support can mean almost anything.
Some vendors expose APIs with highly limited functionality, allowing only basic read access while restricting write operations that are critical for real workflow automation. Others technically support FHIR but expose only a narrow subset of resources that are insufficient for meaningful operational use. Authentication implementations may be inconsistent, awkward, or poorly documented. Sandbox environments may behave very differently from production systems, creating false confidence early in implementation.
Rate limits introduce another hidden problem. An API that works perfectly in testing may become operationally useless once real transaction volume begins flowing through the system.
This creates a dangerous disconnect between commercial assumptions and technical reality.
From the outside, a healthcare platform may appear integration-ready because API access exists.
From the inside, engineering teams may discover that meaningful interoperability requires weeks of architectural workaround design.
That is why successful healthcare integration begins with API maturity validation rather than vendor marketing claims.
Legacy Infrastructure Makes Modern API Projects Much More Difficult
Healthcare technology environments are rarely composed entirely of modern cloud-native systems designed around clean API-first architecture.
Most real organizations operate hybrid ecosystems built over many years, often through incremental software adoption, departmental purchasing decisions, mergers, acquisitions, and reactive modernization efforts.
A hospital network may rely on a legacy EHR with partial API support, laboratory infrastructure built around HL7 messaging, billing platforms with limited connectivity options, telehealth software exposing modern REST endpoints, and internal operational tools developed years ago with inconsistent integration logic.
This creates architectural friction immediately.
Even when one vendor offers clean APIs, surrounding systems may not support the same communication model.
The result is that healthcare API integration often requires translation layers, middleware orchestration, protocol bridging, transformation logic, and compatibility engineering instead of simple direct API consumption.
This is not a failure of APIs themselves.
It is a consequence of the fact that healthcare infrastructure evolves unevenly.
Organizations expecting clean SaaS-style integration experiences frequently underestimate how much engineering complexity hybrid healthcare ecosystems create.
Poor Data Quality Can Break Even Technically Successful Integrations
One of the most underestimated healthcare integration problems has nothing to do with APIs at all.
It is data quality.
An API can function perfectly from a technical perspective while still delivering operational chaos if the information being exchanged is inconsistent, incomplete, or structurally incompatible.
Healthcare data is notoriously difficult in this regard.
Patient names may be entered differently across systems. Date formats may vary. Addresses change over time. Insurance identifiers may be incomplete or outdated. Medication naming conventions may differ depending on coding standards or vendor implementation. Diagnostic terminology may be inconsistent. Clinical notes frequently exist as unstructured free text that machines cannot easily normalize.
Technical connectivity does not solve these issues.
It accelerates their movement.
This creates one of the most expensive mistakes in healthcare integration planning, where leadership assumes API engineering is the primary project while technical teams discover that data normalization, transformation, validation, and reconciliation consume far more time and budget than connectivity itself.
Patient identity management becomes especially critical.
If the same patient exists differently across multiple systems, API integrations may create duplicate records, mismatched histories, inconsistent treatment visibility, and operational confusion that directly impacts care continuity.
This is why serious healthcare integration projects treat identity resolution and data normalization as foundational workstreams rather than secondary cleanup tasks.
Security and Compliance Turn Simple Integrations Into Serious Architecture Projects
Healthcare APIs cannot be treated like standard SaaS business integrations.
The sensitivity of healthcare data changes everything.
Medical records contain diagnoses, prescriptions, treatment histories, laboratory results, personal identifiers, financial details, insurance data, and often highly sensitive protected information that carries strict governance requirements.
Every API connection expands the organization’s attack surface.
Authentication architecture must be designed carefully. Authorization models must reflect real operational roles. Audit logging must provide complete visibility. Encryption standards must be enforced consistently. Consent rules may affect what information can be exposed and when. Third-party vendors introduce additional trust dependencies and compliance exposure.
Unlike lower-risk industries, healthcare organizations cannot deploy integrations quickly and fix governance later.
The architecture must be secure from the beginning.
This slows implementation, increases technical effort, and raises architectural complexity significantly.
That caution is justified because failure carries meaningful legal, financial, and reputational consequences.
Healthcare API integration is never just an engineering task.
It is also a governance and risk management exercise.
Workflow Mismatches Frequently Cause Integration Failure
A technically functioning integration does not automatically create business success.
This distinction is one of the most important realities healthcare leaders need to understand.
Two systems may exchange data successfully while the actual operational workflow remains frustrating, inefficient, or incomplete.
A telehealth platform may successfully retrieve patient information but still disrupt scheduling continuity.
A billing API may synchronize claims data while reimbursement workflows remain inefficient.
A diagnostic integration may technically deliver laboratory results while providers still struggle with timing visibility or workflow usability.
Healthcare interoperability is fundamentally about workflow continuity.
Raw connectivity is only one component.
Organizations that focus exclusively on endpoint integration often solve the wrong problem because they start with technical interfaces instead of operational workflows.
Successful healthcare integration begins by mapping how people actually work, where friction exists, what information must move, when visibility is required, and how workflows depend on timing, context, and access.
API architecture should support workflow design.
Not the other way around.
Vendor Documentation Quality Is Often a Bigger Problem Than Expected
This issue sounds mundane, but it has real financial impact.
Healthcare API documentation quality varies dramatically between vendors.
Some organizations provide mature developer ecosystems with reliable documentation, working examples, authentication guidance, testing tools, sandbox environments, sample payloads, and responsive engineering support.
Others provide incomplete documentation, outdated references, vague implementation guidance, inconsistent error descriptions, and weak technical support.
Engineering teams then spend valuable time reverse-engineering behavior, testing undocumented edge cases, and compensating for poor vendor maturity.
Timelines extend.
Budgets increase.
Confidence declines.
This becomes especially problematic when leadership assumed interoperability would be relatively simple because API access was available.
Vendor technical maturity should be treated as a strategic evaluation factor during procurement and architectural planning.
Ignoring this creates preventable implementation pain.
Scalability Problems Often Appear After the Pilot Phase
One of the most dangerous healthcare integration assumptions is believing that a successful proof of concept guarantees production reliability.
Small pilot environments hide structural weaknesses.
Rate limits may not appear under low traffic.
Latency may seem acceptable until real operational workloads begin.
Error handling may seem sufficient until failure scenarios become frequent.
Monitoring gaps may remain invisible until critical workflows depend on uptime.
Healthcare environments require high reliability because failed integrations can disrupt treatment continuity, billing operations, scheduling workflows, diagnostics visibility, and patient communication.
An integration that looks successful in testing may become operationally unstable under production scale if architecture planning did not account for throughput, retries, resilience, failure recovery, monitoring, and vendor dependency constraints.
Scalability must be considered from the beginning.
Waiting until operational failures emerge creates far more expensive remediation work.
How Strong Healthcare Organizations Solve These Challenges
Organizations that succeed with healthcare API integration do not approach interoperability as a connector deployment exercise.
They treat it as infrastructure strategy.
They validate vendor API maturity before making architecture assumptions. They map workflows before designing integrations. They prioritize data normalization and identity resolution early. They design security architecture before implementation begins. They assume hybrid environments rather than idealized API-native ecosystems. They build monitoring, governance, and long-term operational ownership into the architecture itself.
Many of the strongest organizations also introduce abstraction layers between vendor APIs and internal workflows so vendor changes create less disruption over time.
That architectural discipline creates resilience.
It also creates strategic flexibility.
APIs Matter, But They Are Not the Strategy
Healthcare APIs are critically important.
FHIR adoption, digital health growth, analytics modernization, patient-facing applications, and cloud-native interoperability all depend heavily on API-driven architecture.
But APIs remain tools.
They are not strategy by themselves.
Organizations that struggle often assume technical connectivity automatically creates interoperability.
Organizations that succeed understand the broader reality.
Healthcare API integration requires workflow design, governance discipline, security architecture, identity management, data quality engineering, vendor maturity assessment, and long-term operational ownership.
APIs make interoperability possible.
Architecture makes it successful.



